Imagine Life Without Allergies
The diagnosis of allergies/ The management of allergy by immunotherapy/ The preventive strategies for reducing the effect of allergens.

Lozet Pharma is devoted to the improvement of the quality of life of allergy patients. Our mission is to help our patients and consumers to live and work better, by reducing the effect of allergies, one of the commonest chronic ailments in the world.
 Immunotherapy is currently the ONLY intervention that could potentially alter the natural course of allergic diseases
- World allergy Organ J. 2014; 7 (1): 6
Immunotherapy is currently the ONLY intervention that could potentially alter the natural course of allergic diseases
- World allergy Organ J. 2014; 7 (1): 6
We aim to reduce the economic burden and dependence of the patients and consumers on conventional anti-histaminic and steroid medication.
Responsible & Ethical Medicine :
Our core values are patient focus, integrity, ethical medicine & respect for people. We expect our employees and associates to share our values and act with integrity at all times. Doing what is right for the welfare of our patients and consumers is foremost in our hearts.
Patient Focus :
We focus on the individual, doing what is right for the patients and consumers. We are committed to the highest standard of the ethical medical practice and governance in our work. We are committed to deliver the highest quality medicines and products to our patients and consumers.
To do this we work with our partners and customers to improve healthcare and find new ways to improve our delivery systems.
Management of allergies in early childhood is critical to prevent multiple allergies and asthma.
Managing allergies & its symptoms, patients should try and remove triggers from the environment.
Allergy tests can help you find out what you are allergic to so that you can try to stay away from it.
A condition of unusual sensitivity to a substance or substances which, in like amounts, do not affect others.
Immunotherapy reduces the usage of Steroids and anti-histaminics in Allergies Rhinitis and Asthma.
OARIO BITE is a sugar(Sucrose) free formula and intended as Nutritional supplement for PCOD Women.
ORTUM PRO is a sugar(Sucrose) free formula and intended as food supplement for Pregnant Women. ORTUM PRO Diskettes formula has been designed with Protein
ZANUS KID D is Protein powder with Multivitamin, Multimineral, Lactoferrin, colostrum, DHA, Pre and Pro-biotics.
Allergy is an excessive reaction of the immune system to substances which are normally harmless.
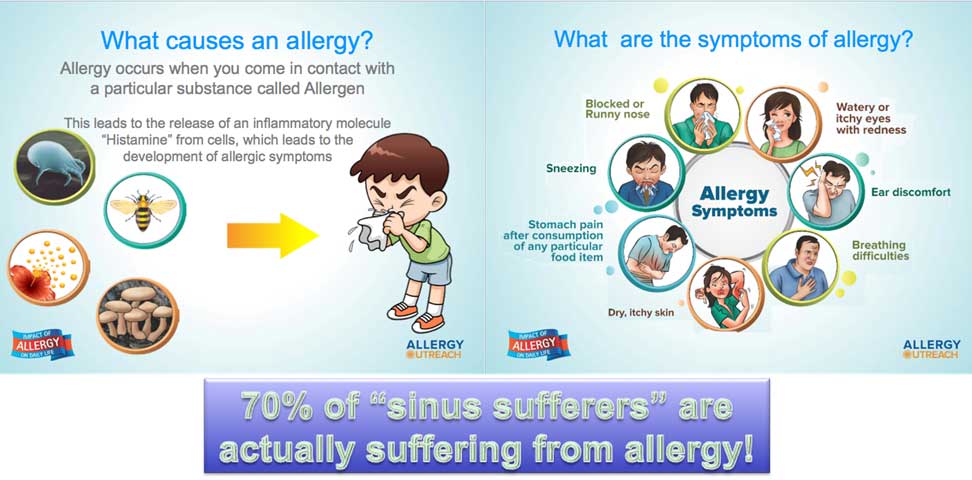
An allergy is a sensitivity to a substance called an allergen. Nasal allergies are most commonly caused by one or more of four kinds of allergens: pollen, house-dust mites, mold, and animals. Because pollen is a problem only during certain times of the year, it usually causes seasonal nasal allergies. House-dust mites, mold, and animals may be around all year long, and so usually cause perennial nasal allergies. Other substances, called irritants, can bother the nose and make allergy symptoms worse.
Allergic asthma often shares the same allergic triggers as allergic rhinitis.
It is important to consider allergy and asthma as the manifestations of a hypersensitive "UNITED AIRWAYS".
The same allergens that give some people sneezing fits and watery eyes can cause an asthma attack in others. Allergic asthma is the most common type of asthma. About 90% of kids with childhood asthma have allergies, compared with about 50% of adults with asthma. The symptoms that go along with allergic asthma show up after you breathe things called allergens (or allergy triggers) like pollen, dust mites, or mold. If you have asthma (allergic or non-allergic), it gets worse after you exercise in cold air or after breathing smoke, dust, or fumes. Sometimes even a strong smell can set it off. Because allergens are everywhere, it's important that people with allergic asthma know their triggers and learn how to prevent an attack.
If you have allergic asthma, your airways are extra sensitive to certain allergens. Once they get into your body, your immune system overreacts. The muscles around your airways tighten. The airways become inflamed and over time are flooded with thick mucus.
Whether you have allergic asthma or non-allergic asthma, the symptoms are generally the same. You're likely to:
Allergens, small enough to be breathed deep into the lungs, include :
Allergens aren't the only thing that can make your allergic asthma worse. Irritants may still trigger an asthma attack, even though they don't cause an allergic reaction.
These Includes :
Your doctor can test you to see what causes your allergic asthma. The two most common (and recommended) methods are :
The second National Heart, Lung, and Blood Institute (NHLBI) guideline on allergic rhinitis & asthma management recommends that all allergic rhinitis & asthma patients who require daily or weekly therapy be evaluated for allergens as possible contributing factors. They also note that, in selected patients with asthma at any level of severity, specific allergy testing may be indicated as a basis for allergen avoidance or immunotherapy.
Nasal allergy medications that don't make you sleepy (like over-the-counter generic Claritin), saline rinses, and decongestant nasal sprays (but only for a few days). If these don't work, use nasal steroid sprays and stronger antihistamines. If none of this helps, it may be time to talk to a doctor about allergy shots.
There are many good asthma treatments, but most require a prescription. These medications include inhaled steroids, which fight inflammation, and bronchodilators, which open up your airways. If traditional treatments don't help your allergic asthma, Xolair, an injectable medication that reduces IgE levels, may help.You may be given an asthma inhaler with albuterol, ipratropium, and/or inhaled steroids (anti-inflammatory agents). You should see a gradual improvement in asthma symptoms over six to eight weeks.